Acute respiratory symptoms are not always a common pediatric respiratory disease: a clinical case report
Los síntomas respiratorios agudos no siempre corresponden a enfermedades pediátricas habituales: reporte de caso clínico
María Teresa Ferri1, Abigail Lima Moncayo2, Andrea Ordóñez Paz3, Santiago Campos-Miño4
Sumary
Background: Respiratory symptoms caused by viral or bacterial agents are highly prevalent among pediatric patients and represent one of the leading causes of visits to the emergency department. Children with asthma or atopic conditions exhibit an increased susceptibility to respiratory infections and often experience a more prolonged disease course compared to those without such conditions. However, various other pathologies can present respiratory symptoms that mimic infectious or allergic etiologies, necessitating a thorough differential diagnosis. Case report: We report a case of a 5-year-old child with asthma and allergic rhinitis who presented to the emergency department with nasal congestion, cough, hypoxemia (SpO2 77%), tachypnea (respiratory rate 43/min), tachycardia (heart rate 129/min), pallor, perioral cyanosis, and intercostal retractions. Physical examination revealed erythematous nasal and oropharyngeal mucosa with white exudates, decreased breath sounds, and the presence of bilateral fine crackles with a peculiar character, featuring an unusually high-pitched tone not observed in previous admissions; wheezing and a prolonged expiratory phase were not present. Initial presumptive diagnosis was a viral acute lower respiratory tract infection; supplemental oxygen and inhaled salbutamol were initiated. However, recent exposure to a poorly ventilated, chlorinated indoor pool and brief submersion with possible aspiration led to a revised diagnosis of chlorine-induced chemical pneumonitis. Treatment with prednisone resulted in clinical improvement. The patient was discharged on day three with salbutamol and continued asthma management. Conclusions: Although chlorine is a well-recognized respiratory hazard, there is a relative scarcity of clinical case reports documenting pneumonitis due to chlorine inhalation in pediatric patients. Given that respiratory symptoms are a frequent reason for medical consultations, healthcare providers are often inclined to consider more common respiratory conditions. However, a thorough clinical assessment remains essential, always keeping in mind alternative diagnoses such as chlorine inhalation to ensure accurate identification and appropriate management.
Keywords: chlorine gas; chlorine inhalation; chemical pneumonitis; pool chemicals; pediatric.
Resumen
Antecedentes: Los síntomas respiratorios son altamente prevalentes en pacientes pediátricos y representan una de las principales causas de consulta en los servicios de urgencias pediátricas. Los niños con asma o enfermedades atópicas presentan una mayor susceptibilidad a infecciones respiratorias y, con frecuencia, experimentan una evolución más prolongada en comparación con aquellos sin estas condiciones. Sin embargo, diversas patologías pueden manifestarse con síntomas respiratorios que imitan etiologías infecciosas o alérgicas, lo que hace necesaria una evaluación diferencial exhaustiva. Reporte de caso: Se presenta el caso de un niño de 5 años con antecedentes de asma y rinitis alérgica que acudió al servicio de urgencias con congestión nasal, tos, hipoxemia (SpO2 77%), taquipnea (43 respiraciones/minuto), taquicardia (129 latidos/minuto), palidez, cianosis perioral y retracciones intercostales. El examen físico reveló mucosa nasal y orofaríngea eritematosa con exudados blancos, ruidos respiratorios disminuidos y la presencia de estertores finos bilaterales de carácter peculiar, con un timbre inusualmente agudo que no se había observado en ingresos previos. El diagnóstico presuntivo inicial fue infección aguda del tracto respiratorio inferior, por lo que se inició oxigenoterapia suplementaria e inhalación de salbutamol. Sin embargo, la exposición reciente a una piscina cubierta con cloración en un ambiente mal ventilado y un breve episodio de inmersión llevaron a una revisión del diagnóstico, identificándose neumonitis química inducida por cloro. El tratamiento con prednisona resultó en una mejoría clínica. El paciente fue dado de alta al tercer día con salbutamol y continuó con su manejo habitual para el asma. Conclusiones: Aunque el cloro es un reconocido agente nocivo para el sistema respiratorio, existe una relativa escasez de informes de casos clínicos que documenten neumonitis por inhalación de cloro en pacientes pediátricos. Dado que los síntomas respiratorios son una causa frecuente de consulta médica, los profesionales de la salud suelen considerar primero las condiciones más comunes. No obstante, una evaluación clínica minuciosa es fundamental, manteniendo siempre en cuenta diagnósticos diferenciales como la inhalación de cloro para garantizar una identificación precisa y un manejo adecuado.
Palabras clave: gas cloro; inhalación de cloro; neumonitis química; químicos en piscinas; pediatría
Pediatric Residency Program, Universidad Internacional del Ecuador; Quito, Ecuador. https://orcid.org/0000-0002-7257-1967
Pediatric Residency Program, Universidad Internacional del Ecuador; Quito, Ecuador. https://orcid.org/0009-0007-1249-297X
Pediatric Residency Program, Universidad Internacional del Ecuador; Quito, Ecuador. https://orcid.org/0000-0002-0936-5044
Director of Clinical Research and Attending Pediatrician, Department of Pediatrics, Hospital Metropolitano; Quito, Ecuador. https://orcid.org/0000-0003-4686-7358
Usted es libre de: Compartir — copiar y redistribuir el material en cualquier medio o formato.
Adaptar — remezclar, transformar y construir a partir del material para cualquier propósito, incluso comercialmente.
Respiratory symptoms caused by viral or bacterial agents are highly prevalent among pediatric patients and represent one of the leading causes of visits to the emergency departmen1. Children with asthma or atopic conditions exhibit an increased susceptibility to respiratory infections and often experience a more prolonged disease compared to those without such conditions2. However, various other pathologies can present with respiratory symptoms that mimic infectious or allergic etiologies, necessitating a thorough differential diagnosis.
Clinical case
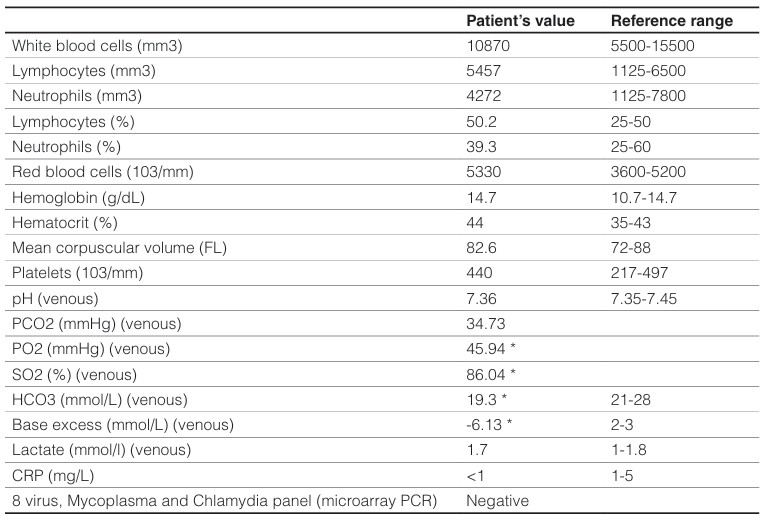
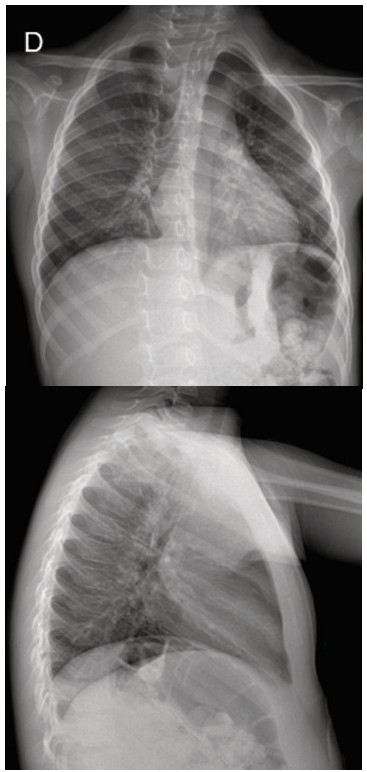
A 5-year-old boy with previous history of frequent admissions for pneumonia and acute asthma presented with 30 hours of nasal congestion and cough. His condition worsened over the last 6 hours, leading to respiratory distress and oxygen desaturation (measured by his mother as <80% at home). The patient's past medical history includes allergic rhinitis and asthma, managed with fluticasone and fexofenadine. There is a history of four previous hospitalizations for acute asthma and pneumonia, the most recent occurring two months ago and treated with antibiotics. His immunization status is incomplete for his age. The parents deny any exposure to tobacco smoke or biomass fuels. On physical examination, his oxygen saturation was 77%, respiratory rate 43/min, and heart rate 129/min. He appeared pale, with perioral cyanosis. The conjunctival, nasal and oropharyngeal mucosa showed erythema. Intercostal retractions were noted along with diminished breath sounds with no wheezing and a peculiar finding of bilateral high-pitched rales. There were no other clinical findings of relevance. Oxygen and inhaled salbutamol (albuterol) were started. Laboratory investigations, including a complete blood count, venous blood gas analysis, C-reactive protein, and a respiratory micro-array PCR panel, were unremarkable, except for a mild elevation in the absolute number of lymphocytes (Table 1). The chest X-ray revealed accentuated bilateral interstitial and peribroncovascular markings (Figure 1).
Table 1. Laboratory test results at admissiondismo (Figura 1). Se complementó estudio con hormona tiroxina libre (FT4) 1.3 ng/dl (normal), hormona tiroxina total (TT4) 13.1 ug/dl (alta) y anticuerpos anti-receptor TSH (TRAb) elevados, con estos resultados se suspende levotiroxina.
En la semana 20 de gestación presentó cuadro de infección por COVID-19 leve. En la semana 27 de gestación por TSH suprimida y presencia de síntomas como diaforesis nocturna, temblor, calor y rubor facial, se inició terapia farmacológica antitiroidea con metimazol 2.5 mg al día.
En último control previo al parto, a la 37 semana de gestación se evidencia TSH 5.07 uUl/ml (elevada), FT4 0,57 ng/dl (baja) y TRAb negativos, se suspendió terapia con metimazol.
A la semana 38 fue parto sin complicación.
En control post parto, a la octava semana valor de TSH 0,14 uUl/ml (baja) con FT4 y TT4 total normal, por lo que se continuó con conducta expectante, a la semana 13 se evidenció valor de TSH 218.5 uUl/ml, FT4 0.18 ng/dl con sintomatología de hipotiroidismo como voz ronca, mialgias, fatiga, intolerancia al frio, edema, incremento de peso, depresión, piel seca, caída de cabello por lo que se instaura suplemento con levotiroxina 150 mcg por 7 días, luego a 100 mcg obteniendo un mejor control con una TSH de 3.38 uUl/ml y mejoría clínica, manteniéndose con levotiroxina a 88 mcg cada día (Tabla 1).
Table 1. Laboratory test results at admissionNote: abnormal values are shown in bold. The reference range values for blood gas analysis are based on arterial samples, while in this case it is a venous sample.
Figure 1. Chest X-ray at admission.Chest X-ray (PA and lateral views) shows a centrally positioned trachea with normal patency. The cardiac silhouette is within normal limits. Pulmonary parenchyma displays adequate expansion. No consolidations or nodular lesions are present. There is an accentuation of bilateral interstitial and peribroncovascular markings. Both costophrenic and cardio phrenic angles are clearly visible. Soft tissues and bony structures appear unremarkable, with no visible abnormalities.
Chest X-ray (PA and lateral views) shows a centrally positioned trachea with normal patency. The cardiac silhouette is within normal limits. Pulmonary parenchyma displays adequate expansion. No consolidations or nodular lesions are present. There is an accentuation of bilateral interstitial and peribroncovascular markings. Both costophrenic and cardio phrenic angles are clearly visible. Soft tissues and bony structures appear unremarkable, with no visible abnormalities.
The patient was admitted to the hospital with a presumptive diagnosis of an acute lower respiratory infection. Oxygen requirement was low (0.5- 1 L/min), respiratory distress was rapidly released and clinical findings consistent with acute asthma were never present. However, the peculiar high-pitched bilateral rales persisted, sounds that were not found in previous admissions and office visits when the patient had respiratory infections or acute asthma. Due to this finding, further investigation was conducted through an interview with the parents, and a key detail emerged: the patient had been participating in daily swimming lessons at an indoor pool with no ventilation. Most notably, on the day the symptoms began, the pool had been freshly chlorinated, just before the lesson and a hard chloride smell was noted. Moreover, during the class, an attempt by the swimming instructor to teach the patient to float resulted in a brief submersion, leading to coughing, red eyes, respiratory difficulty, and the subsequent development of his symptoms. Therefore, the presumptive diagnosis was revised to chlorine-induced chemical pneumonitis and treatment was adjusted by incorporating prednisone. By day 3, the patient maintained adequate oxygen saturation and had been without supplemental oxygen for 24 hours. On physical examination, the respiratory rate averaged 24 breaths per minute (50th percentile for age). Bilateral breath sounds were preserved, with mild fine rales noted. A follow-up chest X-ray revealed mild bilateral thickening of the peribronchovascular interstitium, primarily in the perihilar and basal regions (Figure 2). Given the patient’s favorable clinical status, he was discharged with prednisone, salbutamol and his regular medication regimen. A follow-up consultation after discharge was unremarkable.
Figure 2. Chest X-ray at day 3 of admission.Chest X-ray (PA view) report: cardiac silhouette is within normal limits. Mild bilateral thickening of the peribroncovascular interstitium in the perihilar and basal regions bilaterally. No airway consolidations are observed. Costophrenic and cardio phrenic angles are clear.
Discussion
Respiratory symptoms caused by viral or bacterial agents are highly prevalent among pediatric patients and represent one of the leading causes of visits to the emergency department1. Children with asthma or atopic conditions exhibit an increased susceptibility to respiratory infections and often experience a more prolonged disease compared to those without such conditions2. However, various other pathologies can present with respiratory symptoms that mimic infectious or allergic etiologies, necessitating a thorough differential diagnosis. We present a case of a 5-year-old child with asthma and allergic rhinitis presented to the emergency department with nasal congestion, cough, hypoxemia (SpO2 77%), tachypnea (respiratory rate 43/min), tachycardia (heart rate 129/min), pallor, perioral cyanosis, and intercostal retractions. Examination revealed erythematous nasal/oropharyngeal mucosa with white exudates, diminished breath sounds, and peculiar high-pitched rales, which were not present in previous admissions; wheezing and a prolonged expiratory phase were not present. Initial presumptive diagnosis was a viral acute lower respiratory tract infection; supplemental oxygen and inhaled salbutamol were initiated. However, recent exposure to a poorly ventilated, chlorinated indoor pool and brief submersion with possible aspiration led to a revised diagnosis of chlorine-induced chemical pneumonitis. Treatment with prednisone resulted in clinical improvement. The patient was discharged on day three with salbutamol and continued asthma management.
Approximately 4.500 visits to the emergency department due to chlorine inhalation are reported annually in the United States3. The forms of chlorine associated with respiratory toxicity include chlorine gas, hypochlorous acid, chlorine dioxide, and chloramine4. For pool maintenance chlorine gas is more frequently used. The localization of the lesions caused by inhalation of an irritant chemical product depends on its water solubility. Chlorine gas has intermediate solubility; therefore, it can lead to both upper and lower respiratory tract damage; the main anatomical area affected goes from the nose to the bronchi. The exact mechanism of chlorine-induced respiratory damage is not fully understood. However, it is hypothesized that chlorine gas (Cl2) interacts with the mucus of the respiratory epithelial lining leading to the formation of hydrochloric acid (HCl) and hypochlorus acid (HOCl). Chlorine gas and hypochlorus acid can interact with reactive oxygen species (ROS) such as superoxide (O2−.) and hydrogen peroxide (H2O2) leading to oxidative injury. This process can overstimulate mitochondria to produce more ROS, creating a cycle of cellular injury; studies suggest that this process may be the basis of cardiopulmonary damage due to chlorine inhalation. Furthermore, neutrophils are also recruited by inflammatory mediators, and neutrophil myeloperoxidase can create more HOCl from hydrogen peroxide. Chlorine gas exposure causes overexpression of inducible nytric oxide synthase which produces inflammation and more oxidative stress. This whole inflammatory process generates airway edema, injury, and inflammation, which can result in acute bronchoconstriction and, in some cases, long-term fibrosis and airway hyperreactivity4.
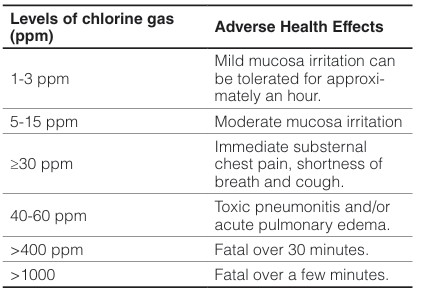
The symptoms of pool chemical exposure range widely, from skin and mucosal irritation to acute respiratory distress and pulmonary edema; depending on factors such as the duration of exposure, the amount and concentration of chlorine involved, the patient’s medical history, and other variables. Regarding chlorine gas levels, humans can detect the odor of chlorine gas at concentrations ranging from 0.1 to 0.3 parts per million (ppm); the health damage that chlorine may cause depends on the level of exposure (Table 2). Notably, studies have shown that the risk of allergic rhinitis and asthma in atopic individuals increases proportionally to their attendance at chlorinated swimming pools4.
Table 2. Health effects depend on the level of chlorine gas.
Adapted from: Achanta & Jordt, 2019
A systematic review was conducted in 1565 symptomatic individuals exposed to chlorine gas; of those, 425 (27%) were due to pool chlorine exposure (median age was 12.5 years). Govier and Coulson (2018) reported a total of 2,407 clinical features, listed in decreasing order: cough, dyspnea, sore throat, eye irritation, excessive sputum or hemoptysis, wheeze, nausea or vomiting, headache, and non-cardiogenic pulmonary edema/acute respiratory distress syndrome (ARDS)5. Death rates range from 1% to 2%, typically due to edema and hemorrhage4. In our patient, pulmonary auscultation revealed bilateral high-pitched rales, an atypical finding in cases of chlorine gas inhalation. Most documented cases report wheezing and diminished breath sounds, whereas high-pitched rales have not been commonly described. This emphasizes the need to include high-pitched rales as a potential clinical sign of chlorine-induced chemical pneumonitis, warranting further investigation and inclusion in the differential diagnosis.
In terms of epithelial repair, bronchial biopsies from humans have demonstrated epithelial desquamation occurring between 3 and 15 days following accidental Cl2 exposure. This is followed by epithelial regeneration, characterized by basal cell proliferation, which begins approximately two months after exposure4.
Currently, there are no established biomarkers for chlorine exposure diagnosis, nonetheless the interest in this field has increased due to the use of chlorine as a chemical weapon in armed conflicts. Recently, the first study of chlorine exposure biomarkers in large mammals was conducted and found palmitoyl-oleoyl phosphatidylglycerol chlorohydrin (POPG-HOCl) and the lipid derivative oleoyl ethanolamide chlorohydrin (OEA-HOCl) in bronchoalveolar lavage fluid (BALF) samples from spontaneously breathing pigs after chlorine exposure. These are formed when chlorine interacts with unsaturated phospholipids present in pulmonary surfactant6.
Conclusions
The differential diagnosis of respiratory illnesses can be challenging due to shared symptoms among various diseases, the need for a thorough clinical examination, accurate interpretation of findings, and reliance on caregiver-reported information. This case emphasizes the importance of considering atypical presentations, as bilateral high-pitched rales, though not classically associated with chlorine-induced chemical pneumonitis, prompted further investigation. Maintaining a broad clinical perspective is essential, as the absence of expected symptoms should not lead to the premature exclusion of potential diagnoses.
Ethical issues
The mother of the patient gave the informed consent for the publication of this clinical case.
Conflict of interest
The authors do not state any conflicts of interest.
Participation of the authors
Conceptualization: SCM, MTF
Collection of references: MTF, AO, ALM
Writing of the manuscript: MTF, AO, ALM, SCM
Revision and final approval: SCM
 https://orcid.org/0000-0002-7257-1967
https://orcid.org/0000-0002-7257-1967